Health and Fitness: The Ups and Downs of Barodontalgia
By LT COL KARL WOODMANSEY, TEXAS AIR NATIONAL GUARD
Imagine that as your aircraft begins to descend, you experience a severe, sharp pain localized in one of your teeth. Such intense pain may distract your focus from the critical details of your flight and may impair your ability to accomplish your mission safely.
Painless teeth can become painful with changes in barometric pressure, cabin pressure, or altitude. Airline passengers typically “pop†their ears to equalize the pressure between their middle ear space and the airplane’s cabin pressure; however, no similar means exist to equalize the pressure between the atmosphere and diseased tooth pulp. The term for this “tooth-squeeze†pain caused by a change in atmospheric pressure is barodontalgia.
Barodontalgia is defined as tooth pain caused by an increase or decrease in ambient pressure. This condition has been reported since the dawn of both flight and undersea exploration but is rarely reported and remains poorly understood. The most common victims are scuba divers because, in deep dives, pressures can increase by several atmospheres (a unit of measure equal to the average air pressure at sea level at 59 degrees Fahrenheit), and military flight crews because of rapid pressure changes. In Airmen, barodontalgia pain may be severe enough to cause premature cessation of flights.
INCIDENCE
Extensive studies have been conducted on military personnel in aircraft, submarine conditions, and hypobaric and hyperbaric chambers. These studies have shown barodontalgia to be a very rare condition, with reported incidence rates between 0.26 percent and 2.63 percent. During their careers, however, barodontalgia is reported to affect 11.9 percent of divers and 11 percent of military aircrews. This percentage translates to a rate of one to two episodes per 200 flight-years.
During World War II, approximately 10 percent of American Airmen experienced one or more episodes of barodontalgia. Overall, barodontalgia prevalence ranged between 0.7 percent and 2 percent in the 1940s, and 0.3 percent in the 1960s. Similarly, 0.3 percent of cases of barodontalgia were reported in high altitude-chamber simulations in the Luftwaffe, which was Germany’s Air Force during World War II. In one recent (2010) study, however, 8.2 percent of 331 Israeli Air Force aircrews reported at least one episode of barodontalgia. Surprisingly, despite advances in aircraft pressurization and dental care—the current in-flight barodontalgia incidence is similar to the incidence in the first half of the 20th century.
One of the first published reports of barodontalgia was in 1937, involving a tooth that became painful at 6,100 feet and required root canal treatment. Barodontalgia has been reported in flights with changes in elevation (and atmospheric pressure) of as little as 3,000 feet, and, in one report, an individual experienced barodontalgia when crossing a 4,000 Âfoot pass in an automobile.
CABIN PRESSURE
Commercial aircraft cabin pressures vary depending on specific aircraft and flight elevation. They are limited, however, by Federal Aviation Administration regulations not to exceed levels equal to an atmospheric pressure of 8,000 feet. Consequently, cabin pressure in commercial aircraft is commonly maintained at levels equal to atmospheric pressure at 3,000 to 8,000 feet. For example, the Airbus A380’s cabin altitude at 43,000 feet is equal to 5,000 feet atmospheric pressure; the Boeing 767’s, is equal to 6,900 feet atmospheric pressure when cruising at 39,000 feet; and the Bombardier Global Express business jet pressurizes to 4,500 feet atmospheric pressure when cruising at 41,000 feet.
Because military aircraft have different needs than commercial aviation, aircraft pressurizations vary greatly depending on aircraft and mission. For example, the C-130 flight station and cargo compartment can be pressurized to maintain a cabin pressure-altitude of 5,000 feet at an aircraft altitude of 28,000 feet, and fighter aircraft cabin altitudes can exceed 10,000 feet.
PRACTICAL
CONSIDERATIONS
- The risk of barodontalgia is very low
- Patients who experience extreme atmospheric pressures are at higher risk
- Healthy teeth have essentially no risk of barodontalgia
- Always rule out referred sinus pain
WHAT CA– USES BARODONTALGIA?
To date, a specific mechanism has not been identified to explain precisely how pressure changes cause barodontalgia pain. Based on published literature, however, two requirements appear necessary for barodontalgia: (1) the ambient pressure must exceed a threshold equivalent to approximately 3,000 feet (or more) of elevation change; and (2) the teeth must have some degree of pre-existing dental disease.
Maintaining optimal oral health is the surest method to reduce the risk of barodontalgia.
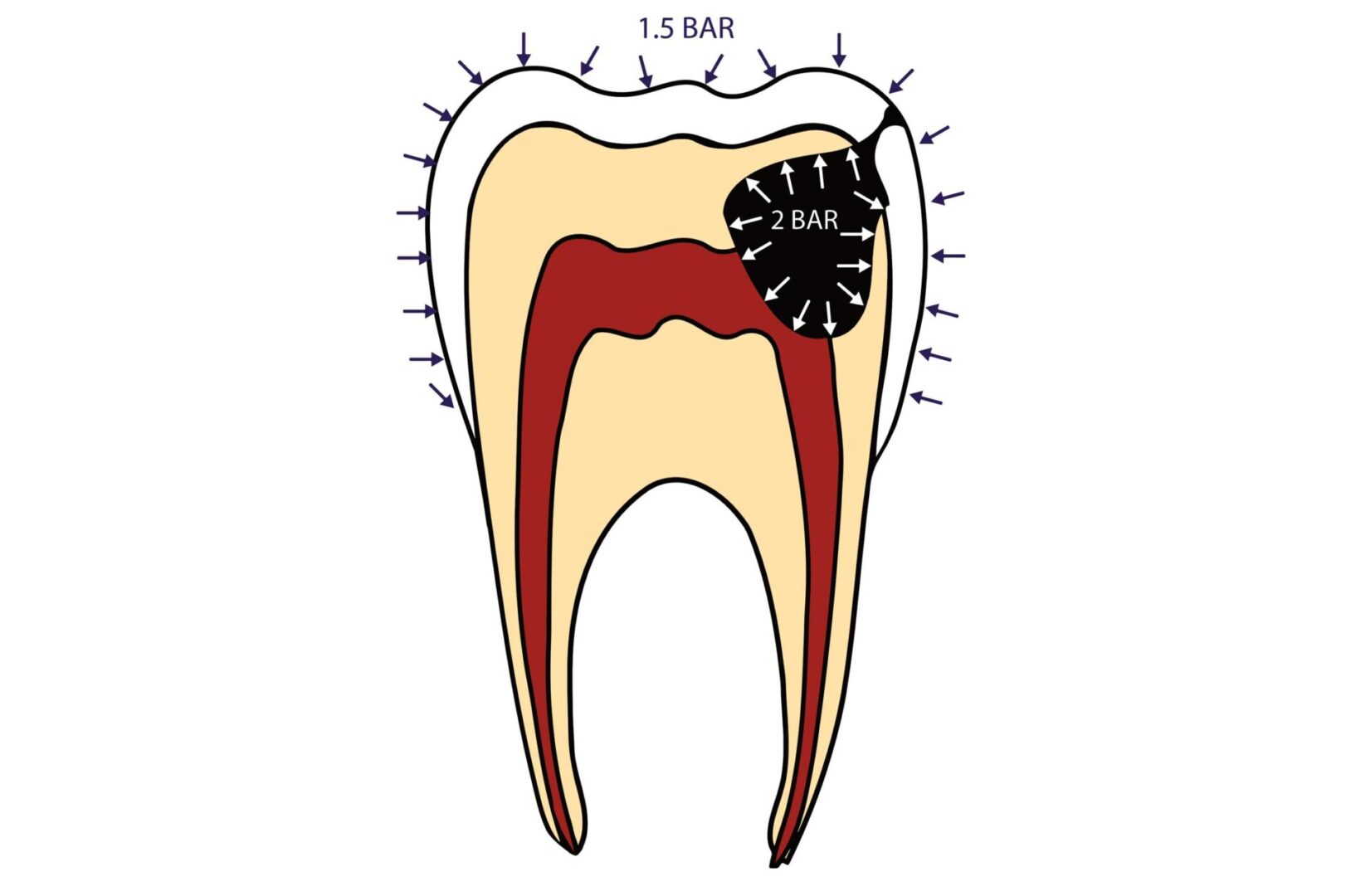
Boyle’s law explains the inverse relationship between gaseous pressure and volume with the formula P1/ V1 = P2/V2. Gases expand when ambient pressure decreases (as it does with increased elevation). Conversely, gaseous volumes shrink when ambient pressure increases. Similar to a barometer, the pulp space inside a tooth reacts to pressure changes. As atmospheric pressures change, the pressure inside the hollow pulp space within the tooth may not be able to equalize pressure. This pressure differential can then trigger the nerves to feel toothache-type pain.
Changes in barometric pressure do not cause dental disease. The pressure changes can provoke a previously asymptomatic diseased tooth to become symptomatic, however. Therefore, barodontalgia is merely a symptom of dental disease. The most common causative dental problems are tooth decay, a defective filling, an abscessed tooth, gum disease, or an impacted tooth.
In some cases, the perceived tooth pain may be referred pain from sinus disease. According to one study, this referred pain may occur in as frequently as 18.5 percent of Airmen reporting barodontalgia-type symptoms. This misconception can be explained by the fact that upper teeth are adjacent to the sinuses and share a nerve pathway to the brain.
AT-RISK POPULATIONS
- Military and civilian pilots, flight crews, and passengers (even parachutists), including aeromedical transport aircrews and patients
- Divers and submariners
- Hyperbaric/hypobaric chamber patients
HOW CAN BARODONTALGIA BE PREVENTED?
Maintaining optimal oral health is the surest method to reduce the risk of barodontalgia. Because nearly all dental disease is preventable, Airmen are encouraged to maintain their oral health with a healthy diet, regular brushing and flossing, and routine professional oral health care. The Air Force Dental Corps is responsible for ensuring the dental health of all Airmen, including aircrew members. Members with disqualifying dental diseases are profiled as “Class 3†and may be restricted from flying. The goal of such classifications is not punitive, but rather to safeguard the Airman, his or her crew members, and his or her aircraft from the risk of barodontalgia.
Aircrew members need to be able to safely concentrate on their mission without the distraction of the nagging pain of a toothache. Although barodontalgia is rarely reported, aircrews should be aware of this condition and maintain their teeth in optimal health to reduce the risk of such distractingly painful incidents.